
Dealing with a skin condition that doesn't just stay on the surface is exhausting. Whether you're scrubbing at stubborn scales or wondering why small red dots suddenly appeared across your chest, Psoriasis is a chronic inflammatory disease where the immune system triggers an overproduction of skin cells. It isn't just a "skin problem"; it's a multisystem issue that can affect your joints and heart if left unchecked. The good news is that we've moved far beyond just using heavy creams. Today, the goal is often complete skin clearance, and for many, that's actually becoming a reality.
Understanding the Different Types of Psoriasis
Not all psoriasis looks or behaves the same. Depending on how your immune system misfires, you'll likely fall into one of these common categories:
- Plaque Psoriasis: This is the most common form, affecting about 80-90% of patients. It shows up as thick, red patches covered with silvery scales. You'll often find these on elbows, knees, and the scalp.
- Guttate Psoriasis: This typically appears as small, drop-shaped lesions. It often hits 8-10% of people and can be triggered by an infection, like strep throat.
- Pustular and Inverse Psoriasis: These are rarer forms. Pustular psoriasis involves white-appearing blisters filled with non-infectious pus, while inverse psoriasis appears in skin folds (like the armpits) and lacks the typical scaling.
It's important to know that psoriasis often travels with "friends." About 30% of people with the condition eventually develop Psoriatic Arthritis, which causes joint pain and stiffness. Because this is an inflammatory disease, there's also a higher risk of cardiovascular issues, making a comprehensive treatment plan vital.
First-Line Defense: Topical Treatments
If your flare-ups cover a small area (usually 2-10% of your body), your doctor will likely start with topicals. These are medications applied directly to the skin to calm inflammation and slow down cell growth.
Standard options include Corticosteroids, which come in various potencies from Class I (strongest) to VII (mildest). While effective for quick relief, using them long-term can lead to skin thinning. To balance this, many use Calcipotriol, a vitamin D analog that helps normalize skin cell production. A newer addition to the toolkit is tapinarof cream, a 1% concentration that has shown promising results in clearing plaques without the side effects of steroids.
Pro tip: If you have a particularly stubborn patch, some dermatologists suggest applying steroids under a bandage (occlusion) to push the medication deeper into the skin, but always check with your provider first to avoid burning the skin.
Scaling Up: Systemic Non-Biologic Medications
When creams aren't enough or the disease is too widespread, it's time for systemic treatments. These are pills or injections that work from the inside out to dampen the overactive immune response.
Traditional options include Methotrexate and cyclosporine. These are heavy hitters but require close monitoring of your liver and kidneys. For those seeking something more modern, oral agents like Apremilast or deucravacitinib offer a way to manage the disease without the intense monitoring required by older drugs.
| Medication | Typical Dose | Primary Goal | Key Consideration |
|---|---|---|---|
| Methotrexate | 10-25 mg/week | Slow skin cell turnover | Liver function monitoring |
| Apremilast | 30 mg twice daily | Reduce inflammation | Generally safer profile |
| Deucravacitinib | 6 mg once daily | Target TYK2 pathway | Higher clearance rates |
The Powerhouse: Biologic Therapies
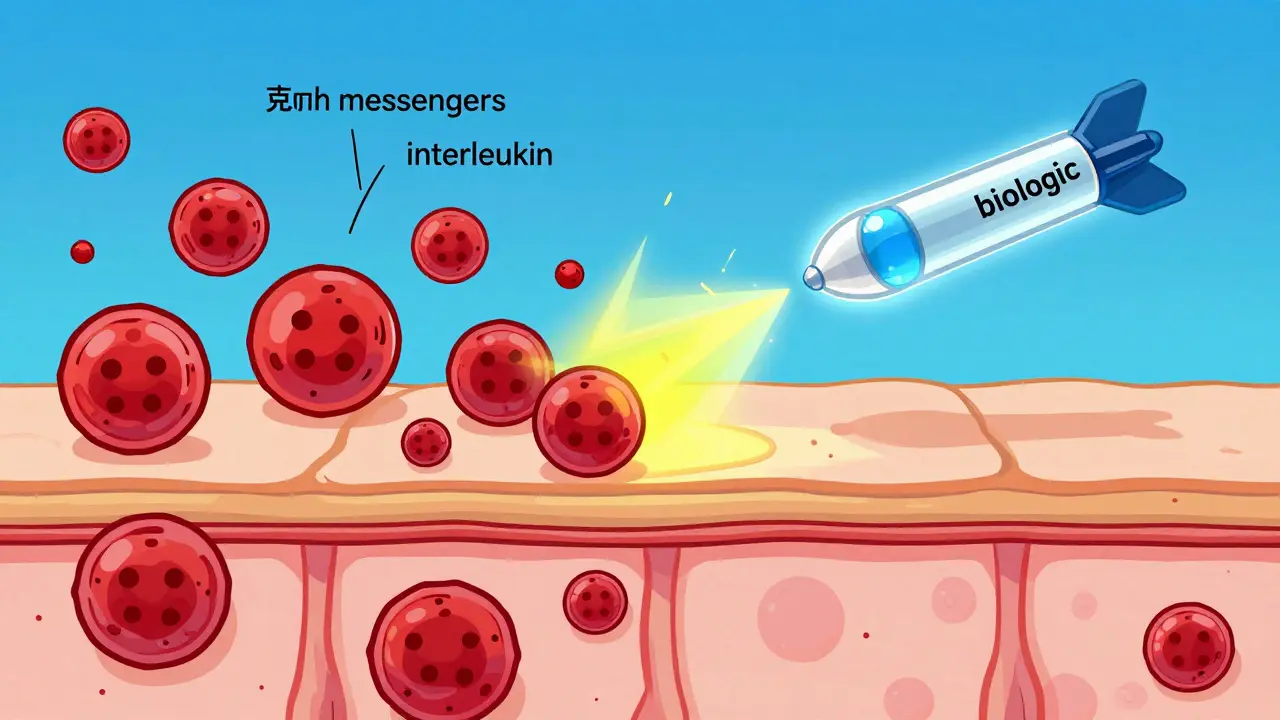
If you've failed traditional systemics, biologics are often the next step. Unlike standard drugs, Biologics are engineered proteins that target specific "messengers" in your immune system. Think of them as precision missiles rather than a blanket dampener.
The biggest breakthrough in recent years has been the shift toward targeting specific interleukins (proteins that signal inflammation). We generally group these into three main camps:
- TNF-α Inhibitors: Drugs like adalimumab were the first big wave. They work well but often require more frequent injections.
- IL-17 Inhibitors: Agents like secukinumab are known for very fast onset. Some patients see significant improvement within just two weeks.
- IL-23 Inhibitors: This is the current gold standard for long-term clearance. Medications like Guselkumab and risankizumab target the "root" of the inflammatory cascade. They are incredibly effective, often achieving 80-90% skin clearance, and the best part is the dosing-some only require an injection once every few months.
For those struggling with scalp or nail psoriasis, IL-23 inhibitors have shown a distinct advantage. Because these areas are hard for creams to reach, a systemic biologic that clears the skin from the inside is often the only way to stop nail pitting or scalp scaling.
Choosing the Right Path: Trade-offs and Tips
Deciding on a treatment isn't just about efficacy; it's about your lifestyle and health history. For example, if you also deal with inflammatory bowel disease (IBD), your doctor might steer you away from IL-17 inhibitors, as they can potentially worsen gut inflammation. In that case, IL-23 inhibitors are usually the safer, preferred choice.
Cost is another major factor. Biologics are expensive, often costing tens of thousands of dollars annually. However, most patients use manufacturer assistance programs to lower these costs. If you're feeling overwhelmed by the paperwork, look for a "Biologics Navigator" or a specialized telehealth service to help speed up the insurance approval process, which can typically take 4-6 weeks.
One final thing to remember: don't get discouraged if the first biologic doesn't work. Research shows that some patients have a "type I interferon" signature instead of the typical "Th17" signature. This means they simply need a different type of drug, not just another brand of the same thing.
How long does it take for biologics to work?
It varies by drug. IL-17 inhibitors are the fastest, often showing a difference in 2 weeks. IL-23 inhibitors typically take about 4 weeks, while older TNF inhibitors can take 8-12 weeks to show significant results.
Can psoriasis ever be fully cured?
While there is currently no permanent cure, newer treatments like IL-23 inhibitors are achieving such high levels of clearance (PASI 90 or 100) that many patients live essentially symptom-free. Some ongoing trials are even testing if early, aggressive treatment can allow patients to stop medication entirely later on.
What is PASI and why does it matter?
PASI stands for Psoriasis Area and Severity Index. It's a tool doctors use to measure how much of your body is affected and how red or thick the plaques are. When you see "PASI 75" or "PASI 90" in medical notes, it means the drug cleared 75% or 90% of the skin, respectively.
Are there risks with long-term steroid use?
Yes. Long-term use of high-potency corticosteroids can lead to skin atrophy (thinning), stretch marks, and a phenomenon called "topical steroid withdrawal," where the skin flares severely once you stop using the cream.
What should I do if I'm not responding to my current biologic?
Talk to your dermatologist about "endotype-specific switching." Instead of just trying another drug in the same class, you may need to switch to a different pathway (e.g., moving from an IL-17 inhibitor to an IL-23 inhibitor) based on your specific immune profile.

